








2018 Summer
An Effective Treatment for Challenging Congestive Heart Failure Cases
Presentation
- A 71-year-old male with a long-standing cardiac condition had undergone four failed cardiac resynchronization therapy (CRT) procedures.
- Two of the failed procedures involved placement of the LV lead by vein using conventional implantation methods, while the other attempts were made with HIS-bundle pacing.
- The patient was referred to MedStar Heart & Vascular Institute to assess the feasibility of undergoing CRT using tools and techniques developed by Seth Worley, MD.
- The patient had also undergone previous bypass surgeries, and was being treated for diabetes mellitus.
Assessment and Diagnosis
- The failed CRT procedures had resulted in refractory congestive heart failure.
- The patient’s overall condition posed no obstacles to attempting another CRT procedure using Dr. Worley’s tools and techniques. The only other option was openheart surgery.
- After being advised of the surgical options and potential outcomes, the patient consented to the CRT procedure.
Treatment
- During the 1.5-hour procedure, a near-total occlusion in the patient’s subclavian vein was dilated using venoplasty.
- At the heart, vessels used in previous lead placements were found to be damaged and blocked.
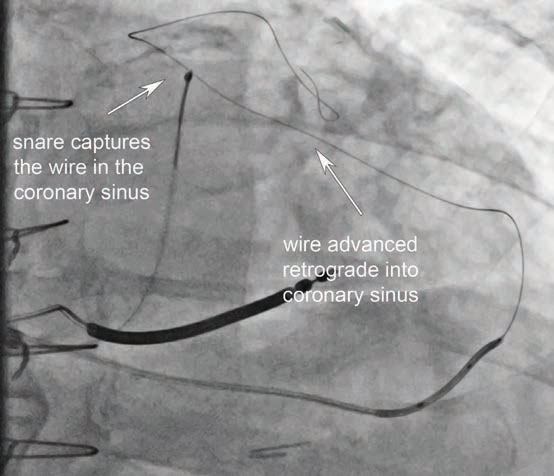
- Access to coronary sinus was achieved using an adjacent, undamaged vein. After widening using venoplasty, the vein was used to successfully place the LV lead using the antidromic snare technique.
- No problems were encountered during the procedure.
Outcome
- Upon awakening from anesthesia, the patient reported feeling immediate improvement.
- Post-operative tests confirmed proper blood flow and left ventricle function. The patient was discharged the day after surgery with no restrictions.
- Patient has continued to show marked progress in his overall health.
Conclusion
- While CRT is a proven treatment for congestive heart failure, the difficulty of placing leads may necessitate the use of alternative techniques.
- The antidromic snare technique is an attractive option in cases where conventional or HIS-bundle approaches are unsuccessful, or the LV lead fails to operate properly.
- The method can also be performed more quickly, reducing the patient’s radiation exposure and anesthesia risks.
- Patients otherwise deemed “too sick” for surgery may nevertheless be candidates for antidromic snare technique procedures.
Dr. Worley says, “Any patient who has had an unsuccessful transvenous attempt at LV lead placement and is being considered for open-heart surgery should first be considered for advanced cardiac resynchronization therapy procedures. As precise placement of the LV lead is a critical factor, methods such as the antidromic snare technique may benefit patients whose congestive heart failure has not improved following CRT procedures that used conventional approaches.”
If you have any additional questions about advanced cardiac resynchronization therapy (CRT) treatment methods, or wish to discuss a patient case, please contact Dr. Worley directly at 202-877-7685, or Seth.Worley@MedStar.net